Clinical Reasoning Corner: Problem Representation
By: Marcela A. de Oliveira Santana and Franco Murillo
Reviewed by: Jack Penner
Welcome back, Clinical Problem Solvers!
Today we are going to talk about the Problem Representation. Let’s go!
Objectives:
Define Problem Representation
Describe the core components of a Problem Representation
Summarize the value of the Problem Representation during the clinical reasoning process
Create a Problem Representation based on data from a clinical case
So, what exactly is a Problem Representation?
A problem representation (PR, or Summary Statement) is an evolving, concise summary that highlights the defining features of a case, helping clinicians generate a focused differential diagnosis and identify the next steps in diagnosis and treatment.
For those who like to use Twitter, you can ask yourself: What if I had to summarize this case and only had one tweet to do it?
The problem representation during the clinical reasoning process
The PR is linked to hypothesis-generation and can act as a guide during the diagnostic journey. It allows clinicians to distill the case into its most relevant features, which facilitates efficient diagnostic schema and illness script selection. As a teaching tool, it helps learners practice identifying key and differentiating case details as they practice and narrate their clinical reasoning.
To create a problem representation you need to be able to abstract critical information from a clinical scenario using semantic qualifiers; for example, young/old, constant/recurrent, diffuse/localized, mild/moderate/severe, and acute/subacute/chronic. By extracting key case details and translating them into generalizable terms, you can more effectively link the case in front of you to your own bank of diagnostic schemas and illness scripts. This will help you identify what new data you need to collect to support or falsify your diagnostic hypotheses.
One more important point: the problem representation is dynamic. It can and should evolve as you gather new information.
Let’s look at a few strategies for constructing a Problem Representation:
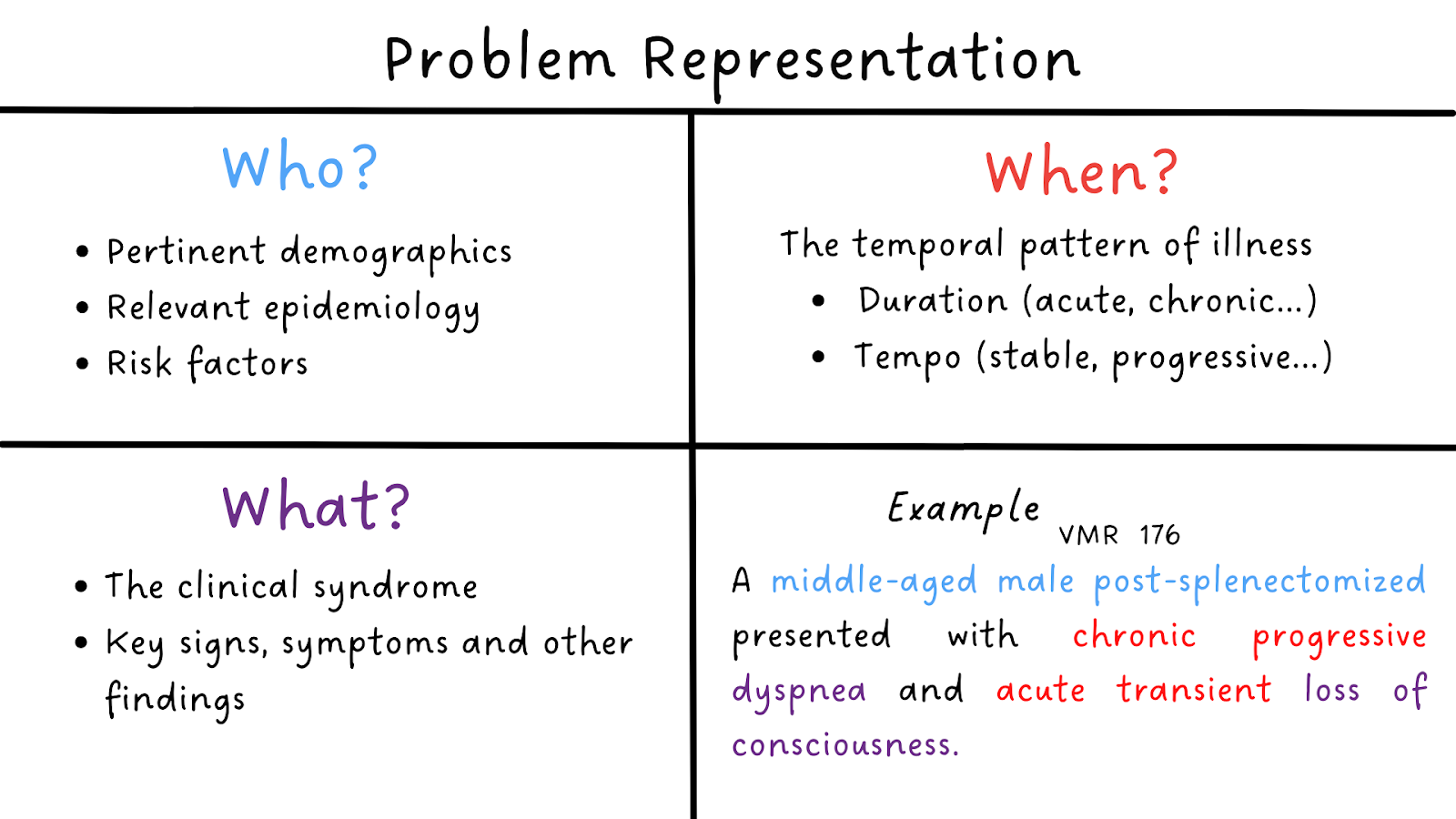
Try to answer 3 main questions in your PR: Who? When? What?
Who is the patient?
Relevant demographics, epidemiology, and risk factors
When did this happen?
The temporal pattern of the illness – the duration (hyperacute, acute, subacute, or chronic) and tempo (stable, progressive, fluctuating)
What is the clinical syndrome?
Key signs, symptoms, and differentiating features of the clinical syndrome.
Also:
Exclude extraneous information – Example: In a patient presenting with fever, cough, and shortness of breath, their history of chronic knee osteoarthritis does not belong in the PR.
Consider what information we need to keep in the background of our mind, not in the initial PR – Example: In a patient presenting with fevers and joint pain, you may not initially include that they have cats/dogs in your PR. However, this may become relevant if you discover in the workup that they have an aortic valve vegetation and negative blood cultures (i.e., culture negative endocarditis). At that point in the case, their exposure to cats can help frame the probability of different organisms that cause culture-negative endocarditis, making it a useful part of your PR.
We often have to pick and choose what to include to avoid overloading the one-liner. The information we include should help us frame someone’s clinical syndrome (e.g., including risk factors for cardiovascular disease in the PR for someone with chest pain).
It is important to understand that each clinician will have their own approach to PR. We should learn that PRs are not “right or wrong”. They can be “better” when all relevant attributes are addressed using the appropriate semantic qualifiers for the specific clinical problem.
Let’s see an example to illustrate what we learned:
You are at the emergency department evaluating a middle-aged male. He reports 3 days of headache, myalgia, and fever. When you hear these initial symptoms, you may not be able to select an illness script because many diseases present with “headache, myalgia, and fever.” However, you can choose between those symptoms and activate the most useful schema to start your diagnostic process. For example, you may start with a fever schema, such as“Fever – Overview” or “Fever – Path to inflammation,” and then examine what diseases on those lists can also present with myalgias and headache,
At this time, your initial PR could be: “A middle-aged male presenting with acute fever associated with headache and myalgia.”
One day later the patient also develops a rash. At this time, you might want to activate another schema, for example, “Fever + Rash”. His past medical history is significant for hypertension and diabetes mellitus. He lives with his wife and 2 cats. He was traveling to Brazil last week to visit some friends, giving you an important clue about the patient’s epidemiological risk and prompting you to think about a new schema: “Fever in a Returning Traveler”.
His labs show leukopenia, lymphopenia, and thrombocytopenia.
At this moment, you can go back to your PR:
“A middle-age male with HTN, diabetes, and recent travel to Brazil presenting with acute headache, myalgia, fever, and rash and found to have leukopenia, lymphopenia, and thrombocytopenia”
Our PR helped us select two schemas (Fever in a Returning Traveler and Fever + Rash). We can look for diseases that may be present in one or both schemas to help identify which illness scripts to compare against the patient’s script.
In this case, we see that Dengue is a differential diagnosis present in both the schemas. You compare the PR with the illness script for Dengue and notice that they match, guiding you to order the confirmatory exams for the final diagnosis.
Final PR:
“A middle-age male with HTN, diabetes, and recent travel to Brazil presenting with acute headache, myalgia, fever, and rash and found to have leukopenia, lymphopenia, and thrombocytopenia. A positive NS1 test result confirmed the final diagnosis of Dengue.”
That covers it, Clinical Problem Solvers! Don’t forget to check the Clinical Reasoning BootCamp VMR episode about the problem representation and see a great example of how the problem representation evolves during the case presentation!
Summary:
A problem representation is a summary that highlights the defining features of a case and will guide you through the clinical reasoning process
It allows clinicians to use pattern recognition to quickly develop a differential diagnosis and allows learners to develop their reasoning skills.
The problem representation is dynamic. It would evolve as soon as you get clinically relevant information.
When you are making a problem representation try to answer 3 main questions: Who? When? What?
References:
Problem Representation Overview. CLINICAL REASONING EXERCISES. JGIM. https://www.sgim.org/web-only/clinical-reasoning-exercises/problem-representation-overview#
Diagnostic Schema. CLINICAL REASONING EXERCISES. JGIM. https://www.sgim.org/web-only/clinical-reasoning-exercises/diagnostic-schema#
- Principles and Practice of Case-based Clinical Reasoning Education A Method for Preclinical Students by Olle ten Cate, Eugène J.F.M. Custers, Steven J. Durning (eds.)
- Denise M. Connor. Key Clinical Reasoning Concepts. Developing Medical Educators of the 21st Century, San Francisco, CA . Feb 25-27,2019. https://meded21.ucsf.edu/sites/g/files/tkssra796/f/wysiwyg/W04%20Handout.pdf
- Martin M, Sedighi Manesh R, Henderson MC, Critchfield JM. Diagnostic Scheming. J Gen Intern Med. 2015;30(12):1874-1878. doi:10.1007/s11606-015-3478-0
- Minter DJ, Manesh R, Cornett P, Geha RM. Putting Schemas to the Test: An Exercise in Clinical Reasoning. J Gen Intern Med. 2018;33(11):2010-2014. doi:10.1007/s11606-018-4599-z