By: Franco Murillo
Reviewed by: Jack Penner
Welcome back, Clinical Problem Solvers.
Today we are going to talk about Illness scripts! So let’s dive in!
Objectives:
1.- Define an illness script
2.- Describe the core components of an illness script
3.- Demonstrate the utility of an illness script in clinical reasoning
4.- Practice applying an illness script as a learning tool
What is an Illness script?
An illness script is a clinical reasoning tool used by clinicians to collect and retrieve clinically relevant information about a particular condition.
In the reasoning process, we use illness scripts to compare and contrast a patient’s clinical presentation (i.e., the patient’s “script”) against our own mental models of a disease (i.e., our own illness scripts) as we reason to a working diagnosis or a final diagnosis.
Perhaps most importantly, illness scripts are dynamic and evolve as we get more exposure to the condition through our own clinical encounters or by hearing or reading about others’ cases. So the illness script we developed as a first-year medical student will evolve over time. Also, illness scripts are specific to each person, so your illness script for a condition will likely have some differences compared with your colleagues’ (we all think and store information in different ways).
How is an illness script organized?
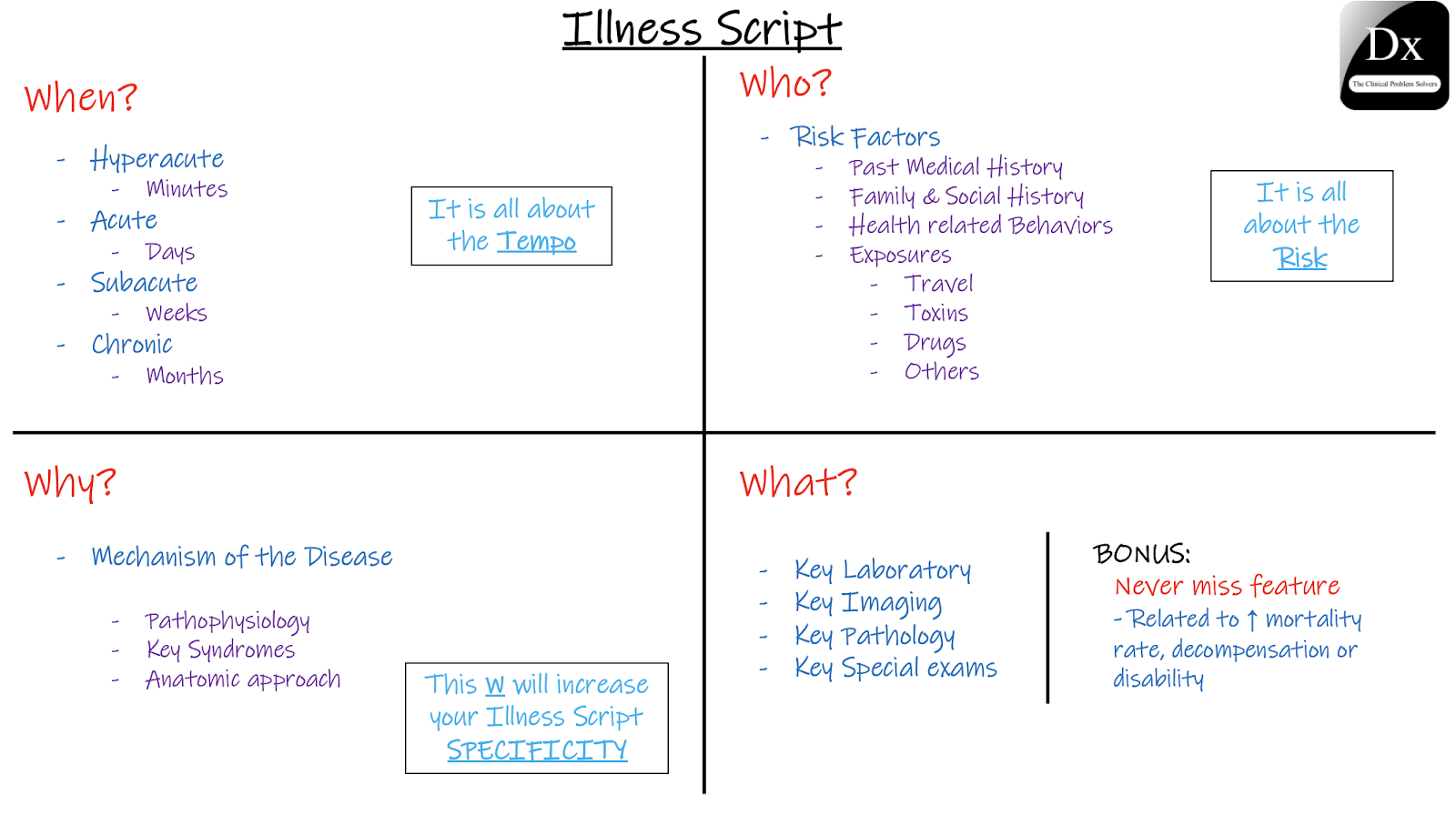
The data gathered on an illness script can be organized into different categories. One helpful organization we use are the 4 W’s + Never miss):
When: It’s all about the tempo
Who: It’s all about the risk factors & exposures.
Why: The disease mechanism. This will solidify your knowledge of the condition and increase the utility of your Illness script.
What: Key diagnostic findings of the disease (e.g., lab tests, imaging, and/or pathology).
Bonus “Never miss”: features linked to increased mortality and morbidity if the disease is missed.
So let’s review our 4 W´s approach and what better way to do it than with a schema about it:
Important: you can always add more categories, but remember that one of the purposes of an Illness script is to be a concise tool that allows you to identify distinguishing features of a disease and compare and contrast different diseases. So, a simple approach, organized in categories that we use to reason through cases will help keep your illness scripts practical and memorable.
How to fill the 4 W´s?
When we want to make our own illness script, we have to decide how we fill each of the 4 W’s. Sometimes this can be challenging because there is so much information available and many diseases have overlapping features (e.g., shortness of breath is present in heart failure and pneumonia). One strategy to optimize the utility of your illness script is to include a key or defining features of a disease that help us distinguish it from others that may have a similar presentation (e.g., elevated jugular venous pulse and an S3 in heart failure, fever cough, and CXR infiltrate in pneumonia). Including key features with high likelihood ratios will help you decide whether to treat, test for, or toss a diagnosis. (Take a look at this post regarding Likelihood ratios for more detailed information. (https://clinicalproblemsolving.com/2020/02/09/clinical-reasoning-corner-likelihood-ratios/).
Let’s practice with a case of Thrombotic Thrombocytopenic Purpura:
Using or 4 W’s approach
What:
Key feature: a feature that is present consistently and ideally exclusively in the condition. For example, reduced activity of ADAMTS 13 and/or presence of ADAMTS 13 autoantibodies in TTP.
Differentiating feature: a feature shared among other similar conditions but not present in many diseases. For example, schistocytes in TTP and other MAHAs.
Things to keep in mind while developing an illness script:
Always prioritize QUALITY over quantity. Not all the W´s need to be filled all the time.
An Illness script is DYNAMIC. You can always update it as soon as you gather more useful info.
Illness scripts VARY from person to person; not everyone stores and uses the information the same way!
Example
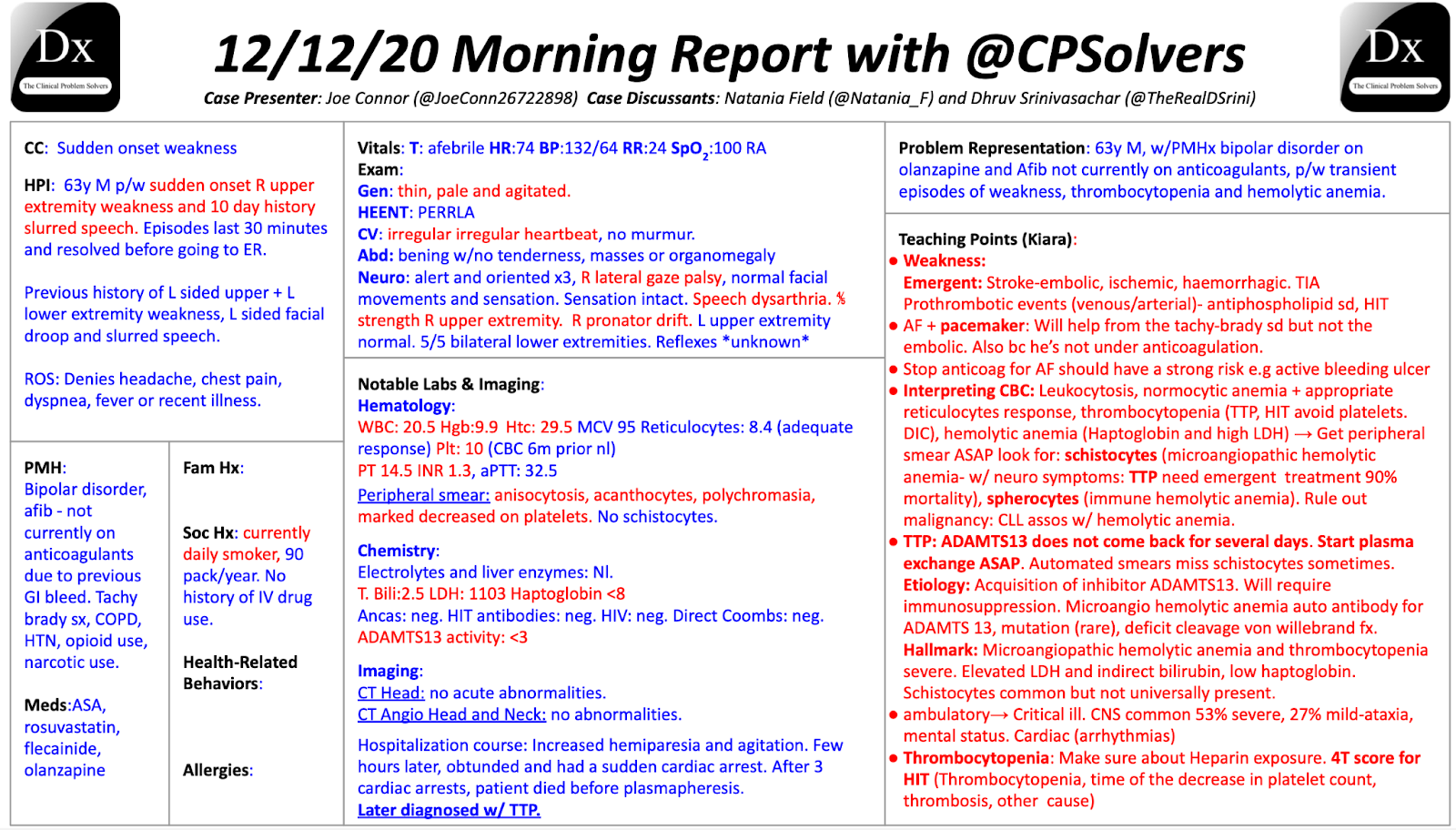
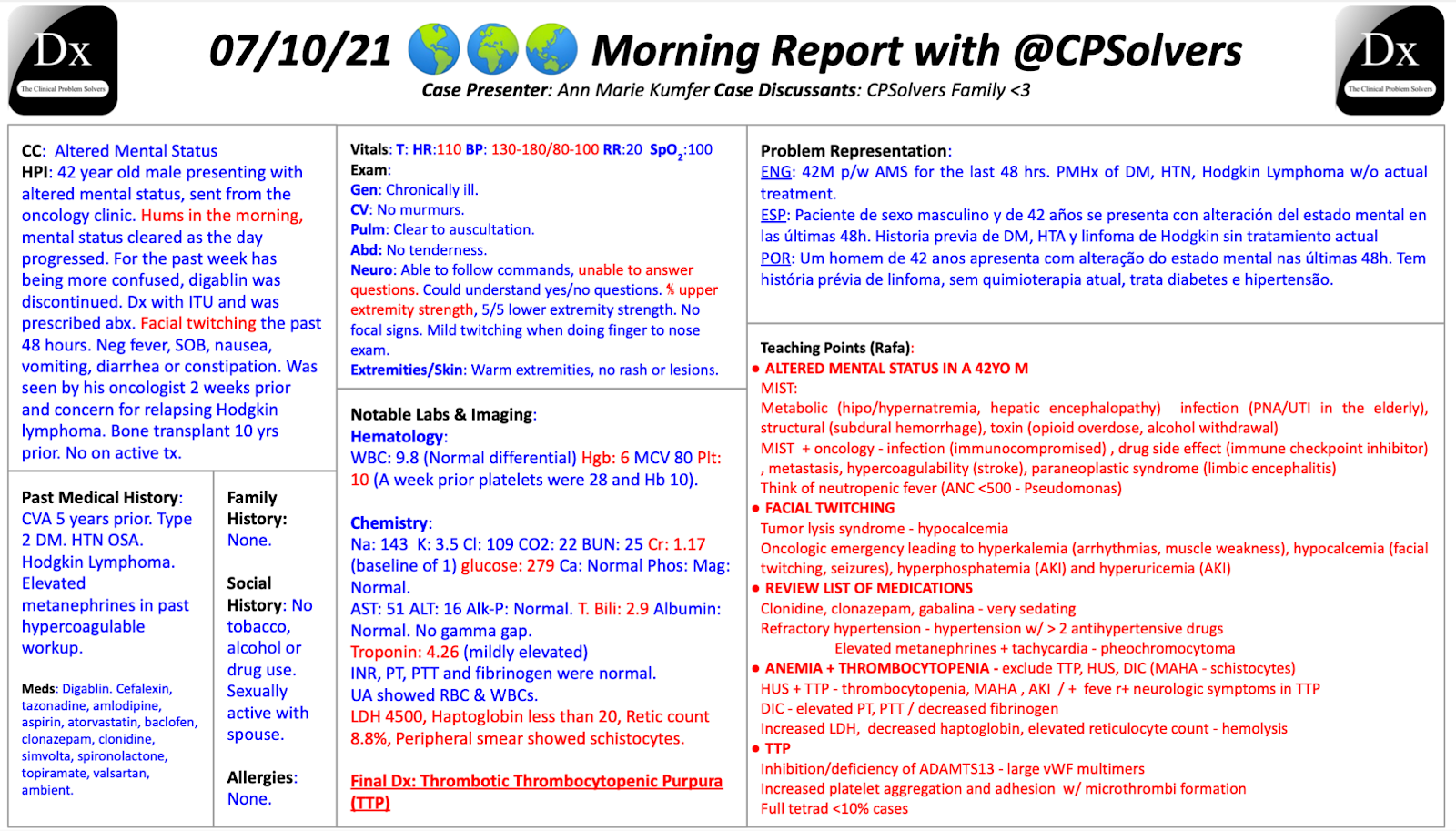
Let’s review an example from some amazing VMR sessions and start building an illness script for TTP.
First, we will use our previous knowledge of TTP and write our first set of W’s
When: Subacute but can deteriorate in a hyperacute fashion
Who: Most common in adults in their third and fifth decade. Common risk factors: PMHx of Lupus, Cancer, or HIV
What: Thrombocytopenia (often <30), schistocytes, neurologic symptoms (Most common)
Why: Reduced activity of ADAMTS 13 with or without detectable autoantibodies, with the formation of small-vessel thrombi that cause MAHA, thrombocytopenia, and risk of organ damage.
You might notice that this version of the Illness script is missing some things discussed during the VMRs. As we said before, more exposure to the disease should prompt us to revisit and update our previous script.
Now, we will incorporate some of the new info we learned during the VMR into our Illness script:
When: subacute but can deteriorate in a hyperacute fashion
Who: Most common in adults in their third and fifth decade. Common risk factors: PMHx of Lupus, Cancer, or HIV
What: Severe Thrombocytopenia (often <30) + MAHA (Increased LDH, Indirect Bilirubin, and low haptoglobin), Schistocytes (Can be missed by automated smears), neurologic symptoms (most common), AKI, fever, and abdominal pain (full tetrad of symptoms present only in 10% of cases)
Why: Reduced activity of ADAMTS13 (presence of large vWF multimers) with or without detectable autoantibodies, formation of small-vessel thrombi that cause MAHA + thrombocytopenia with risk of organ damage and elevated mortality (up to 90%) without treatment.
Never miss: Start treatment (Steroids, Plasmapheresis) ASAP. ADAMTS13 levels will take a while to return.
As you can see, we updated our initial illness script with teaching points from both VMRs. Feel free to do the same for yours! Here is Rabih´s Illness script about TTP for you to use as an example:
Summary:

An Illness script is a powerful tool to store information about key features of different diseases.
It benefits the most from clinical categories that can be useful to compare and contrast when facing a specific symptom, syndrome, laboratory alteration, or imaging finding.
They are dynamic and should be updated as we gather more information about the disease.
They benefit from your creativity to make them our own and memorable!